Introduction
An ascending aortic aneurysm occurs when the portion of the aorta closest to the heart bulges beyond its normal diameter. While many aneurysms grow slowly, reaching a critical size increases the risk of life-threatening complications such as dissection or rupture. Understanding the size thresholds for surgery, along with individual risk factors and recovery planning, empowers patients and families to make informed decisions.
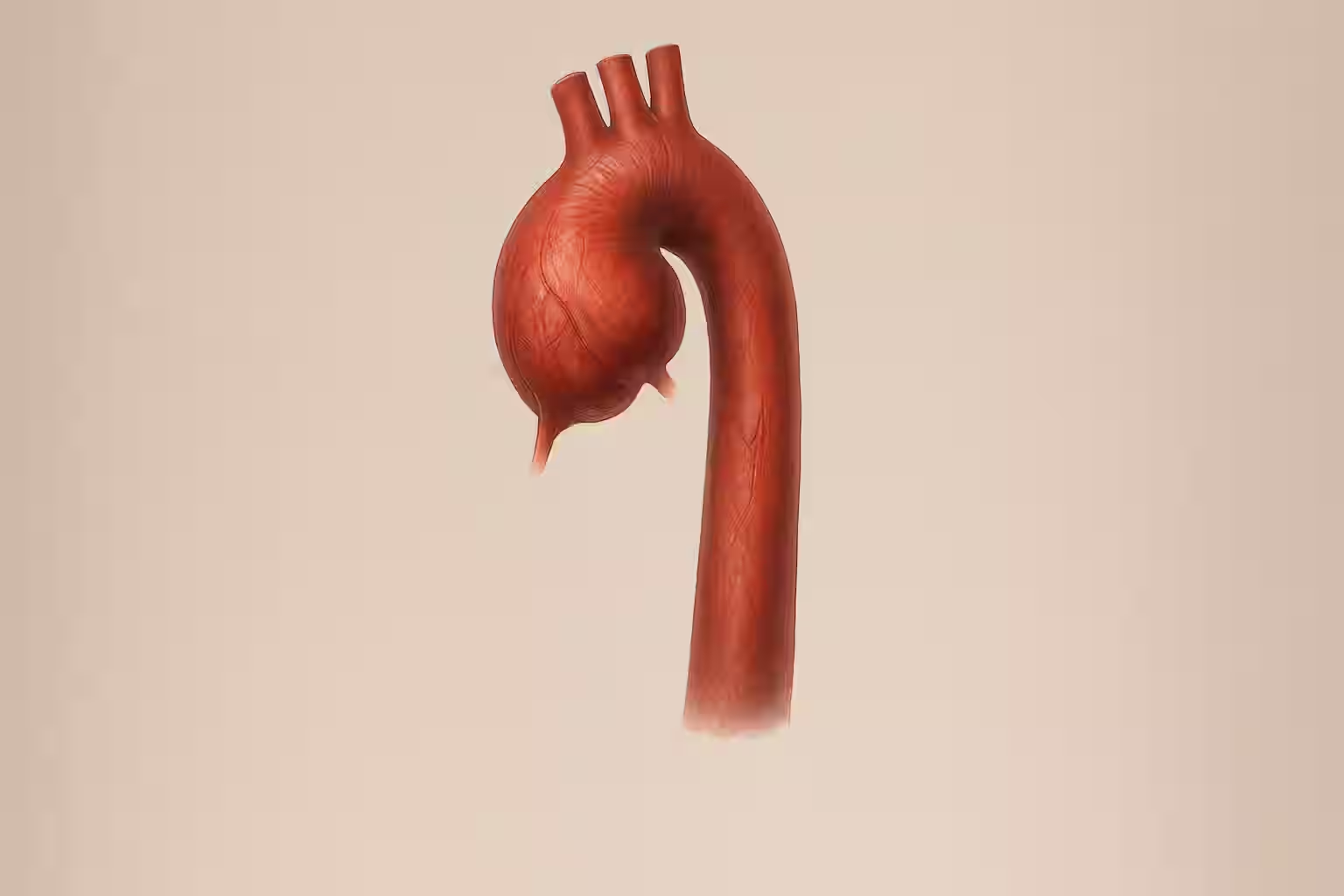
What Is an Ascending Aortic Aneurysm?
An ascending aortic aneurysm is a dilation of the first segment of the aorta. Normally up to 3.5 cm in diameter, an aneurysm is diagnosed when the aorta exceeds 4 cm. Risk factors include hypertension, genetic disorders (e.g., Marfan syndrome), bicuspid aortic valve, and age-related degeneration.
Size Thresholds Guiding Surgery
Standard Recommendations
- 5.5 cm for patients without additional risk factors
- 5.0 cm if there’s a bicuspid aortic valve or family history of dissection
- 4.5 cm in patients with connective tissue disorders (e.g., Marfan, Loeys-Dietz)
Individualized Considerations
- Rapid growth (>0.5 cm/year) may warrant surgery at smaller sizes
- Symptoms such as chest pain or shortness of breath
- Coexisting cardiac conditions (e.g., valve disease)
Assessing Growth Rate
Imaging Modalities
- Echocardiogram: First-line for monitoring diameter
- CT angiography or MRI: Detailed evaluation for borderline cases
Monitoring Schedule
- Aneurysms 4.0–4.4 cm: Imaging every 12 months
- Aneurysms 4.5–5.4 cm: Imaging every 6 months
Surgical Options
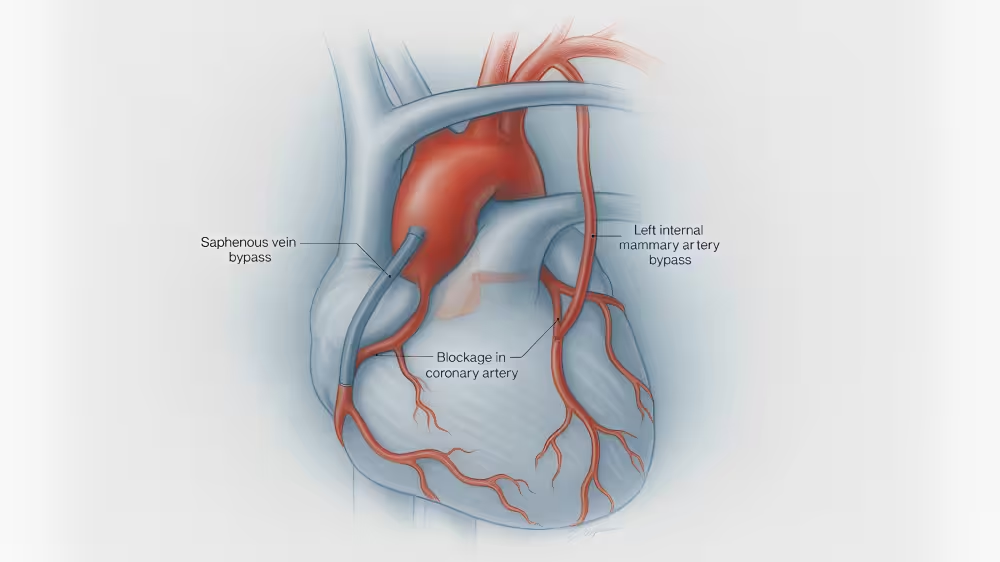
Open Surgical Repair
- Replacement of the aneurysmal segment with a synthetic graft
- Gold standard for most patients
Endovascular Repair (TEVAR)
- Less invasive, deploying a stent graft inside the aorta
- Reserved for those with suitable anatomy or high surgical risk
Post-Operative Recovery
Sternal Precautions
- No lifting >10 lbs for 6–8 weeks
- Use pillow to brace when coughing
Driving and Flying
- Avoid driving until off narcotics and cleared by surgeon (usually 4 weeks)
- Commercial flights discouraged for at least 2 weeks
Activity Progression
- Cardiac rehabilitation: Begins 4–6 weeks post-op
- Gradual return to aerobic activities at 12 weeks
Long-Term Follow-Up
- Lifelong imaging every 1–2 years
- Strict blood pressure control with beta-blockers or ARBs
- Regular cardiology visits
Conclusion
Deciding when to operate on an ascending aortic aneurysm hinges on precise size thresholds, growth rate, and individual risk factors. Early detection and timely surgery can prevent catastrophic complications. If you or a loved one has been diagnosed with an ascending aortic aneurysm, seek a second opinion with Verus to ensure personalized, expert guidance.
Ready to get started? Learn more about our process and request your second opinion at My Verus Report.