Introduction
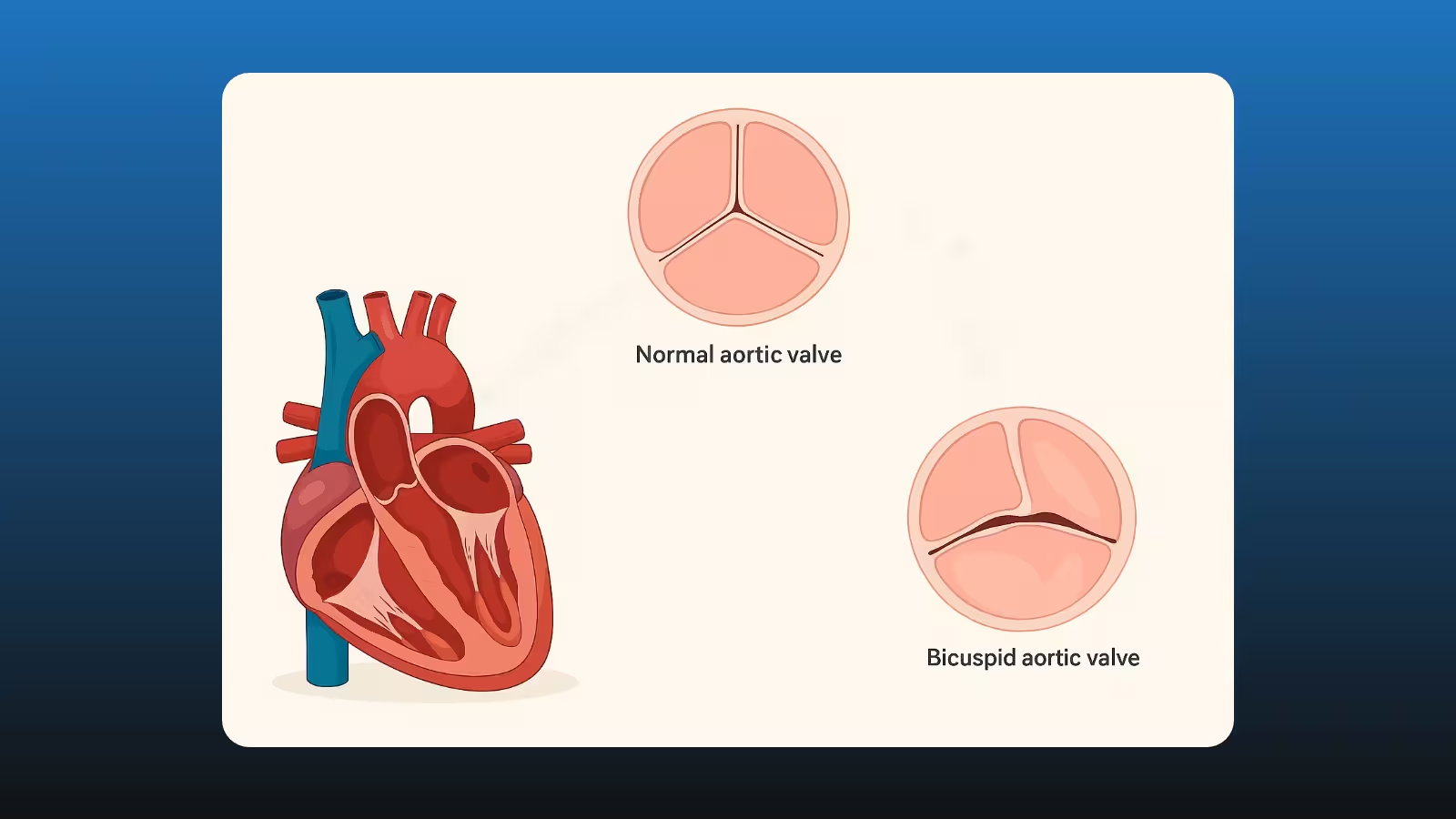
A bicuspid aortic valve (BAV) is a common congenital heart defect affecting 1-2% of the population. Instead of three leaflets, the valve has two, predisposing patients to early valve dysfunction and aortopathy - dilation of the ascending aorta. Deciding when to operate involves balancing risks of surgery against risks of complications like heart failure or aortic dissection.
Anatomy and Pathophysiology
What Is a Bicuspid Aortic Valve?
In BAV, two valve cusps fuse, altering blood flow and causing turbulence. Over time, this leads to valve stenosis or regurgitation and weakening of the aortic wall.
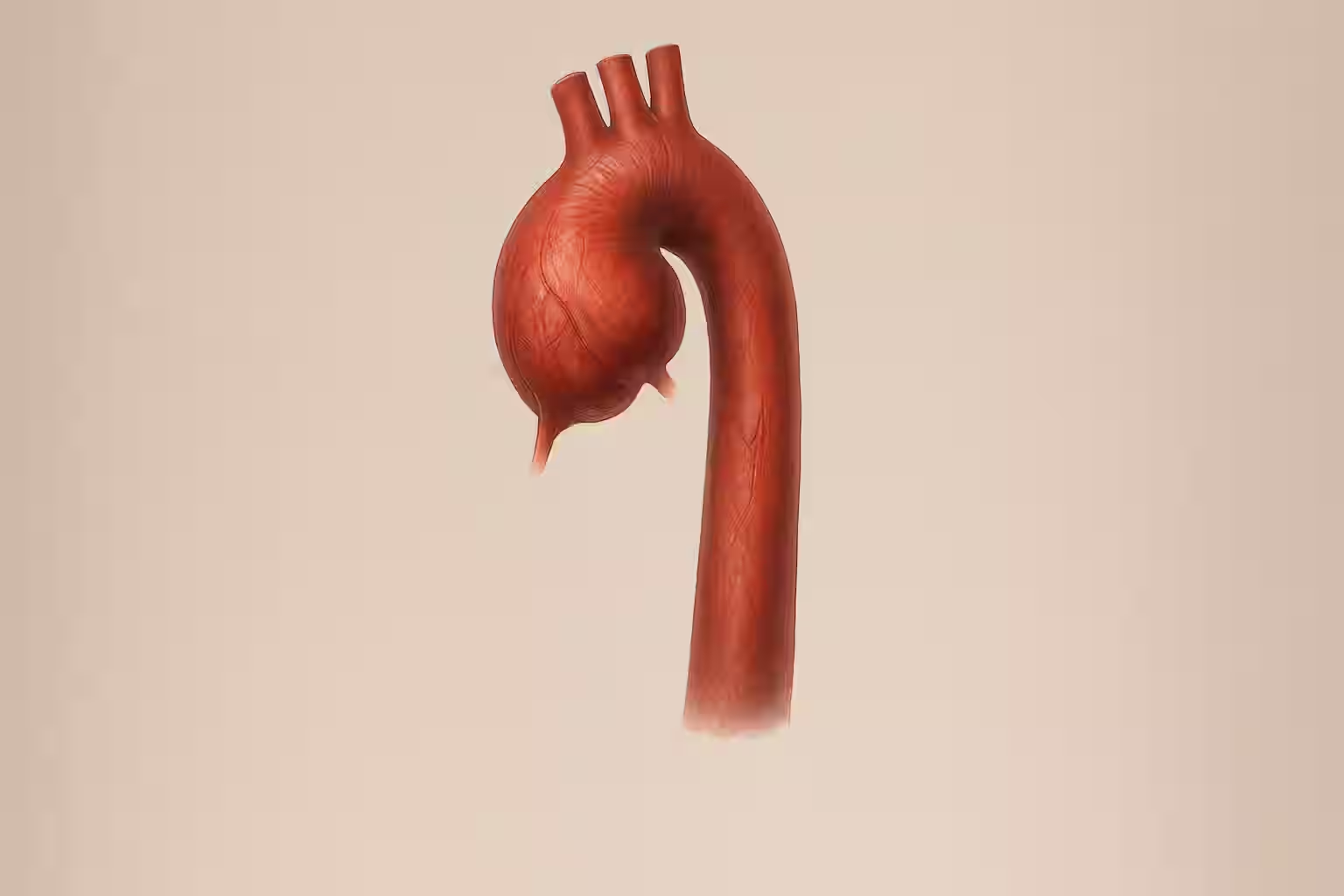
Aortopathy: Beyond the Valve
Up to 50% of BAV patients develop ascending aortic aneurysms due to abnormal connective tissue and shear stress. Aneurysm growth increases risk of dissection or rupture if left unchecked.
Indications for Surgery
Valve Disease Criteria
Surgery for severe aortic stenosis is advised when the valve area <1.0 cm² or mean gradient >40 mmHg with symptoms; for regurgitation when left ventricular dilation or reduced function occurs.
Aortic Size Thresholds
Elective repair is recommended when the ascending aorta diameter ≥5.0 cm in BAV patients, or ≥4.5 cm if there are risk factors (family history of dissection, rapid growth >0.5 cm/year).
Combined Valve and Aorta Surgery
If valve surgery is indicated and aorta diameter ≥4.5 cm, simultaneous ascending aorta replacement reduces future risk.
Procedural Options
Valve Repair vs Replacement
Valve repair preserves native tissue when anatomy allows, yielding better long-term outcomes and no need for lifelong anticoagulation. Replacement uses mechanical or bioprosthetic valves, chosen based on age, comorbidities, and patient preferences.
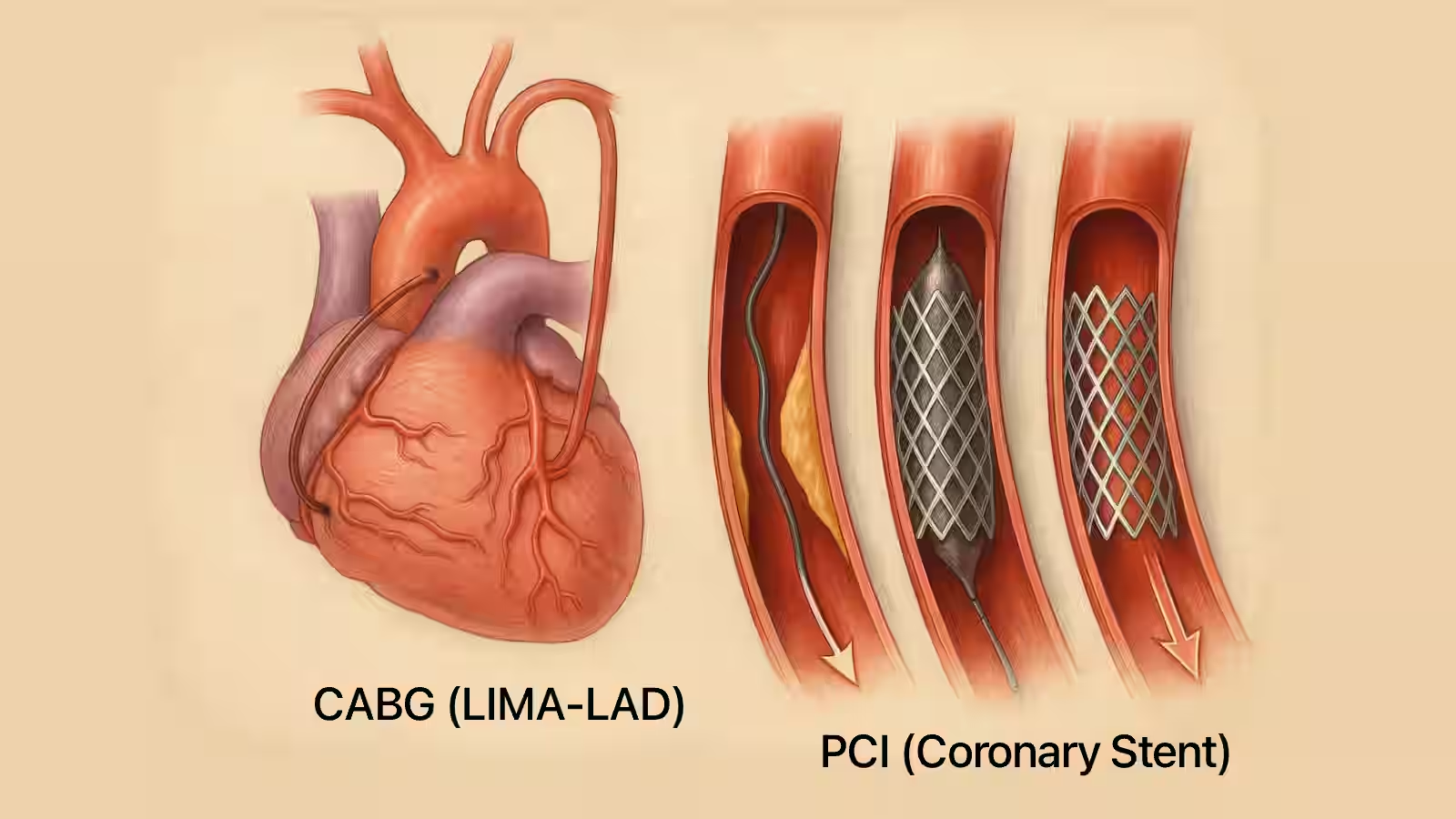
Aortic Replacement Techniques
- Tube graft replacement of ascending aorta
- Valve-sparing root replacement (David procedure) for patients with minimal valve dysfunction
- Composite graft (Bentall) when significant root dilation and valve disease coexist
Recovery and Precautions
Sternal Precautions
Avoid lifting >10 lbs, pushing, or pulling for 6-8 weeks. Use support when coughing.
Driving and Flying
Long-Term Follow-Up
Annual imaging with echocardiogram and CT/MRI surveillance of aorta growth, plus cardiology visits every 6–12 months.
Conclusion
Timely surgery for bicuspid aortic valve and aortopathy can prevent life-threatening complications and improve quality of life. A heart team approach ensures tailored decisions for each patient.
Ready for a second opinion? Learn more about our expert cardiac review services and schedule your consultation today.